


CHIEF COMPLAINT:
Trauma activation.
HISTORY OF ILLNESS:
Upon the paramedics arrival, his GCS was reported as 10, he had some sonorous on his respiration, it was felt that he was not particularly protecting his airway well. He was intubated using only succinylcholine and lidocaine. He was transported to the emergency department with stable vital signs en route.
HISTORY OF ILLNESS:
I was called to 5-ICU to intubate this gentleman with recent significant head injury. However, he was extubated yesterday. This evening he developed increasing respiratory difficulty with retractions, tachypnea and increased restlessness.
EMERGENCY DEPT. COURSE:
The patient was triaged to room 14 and met the paramedics upon arrival. They did arrive code 3 as full trauma activation. This is the patient that appears to primarily have had a traumatic brain injury. The patient will be admitted to the intensive care unit for further neurological monitoring. The patient is admitted in critical condition.
FINAL DIAGNOSIS:
1. Traumatic brain injury.
2. Respiratory failure.
3. Abrasions.
CONSULTATION CHIEF COMPLAINT:
Caucasian man status post head injury with aspiration risk. PEG (percutaneous endoscopic gastrostomy) feeding tube is requested for nutritional purposes and for adminisrtation of medications.
HISTORY OF ILLNESS:
The patient had decreased mental status and a closed head injury requiring intubation/protection of airway, and eventual tracheostomy placment. The patient has had evidence of partial right hemiparesis and continued decreased mental status. He has had NG tube for administration of medications. Patient has pulled out his NG tube on numerous occasions. Swallowing studies have shown significant aspiration risk. PEG placement is therefore being requested for administration of medications as well as for nutritional purposes.
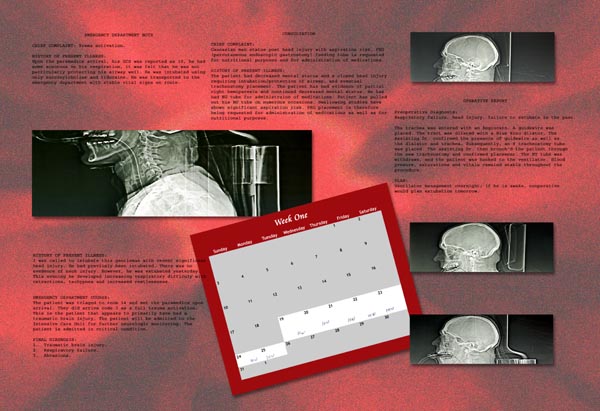
Preoperative Diagnosis:
Respiratory failure, head injury, failure to extubate in the past.
The trachea was entered with an Angiocath. A guidewire was placed. The tract was dilated with Blue Rhino dilator. The assisting Dr. confirmed the presence of guidewire as well as the dialator and trachea. Subsequently, an 8 tracheostomy tube was placed. The assisting Dr. then bronch’d the patient through the new tracheostomy and confirmed placement. The ET tube was withdrawn, and the patient was hooked to the ventilator. Blood pressure, saturations and vitals remained stable throughout the procedure.